Everyone loves Henrik Lundqvist. No seriously, everyone. I'm an Islanders fan and I can't but find him likable. He's one of the best goaltenders in the game.
On January 31st in a game against the Carolina Hurricanes, Rangers defenseman Ryan McDonagh attempted to clear the crease. Doing so, McDonagh's stick inadvertently came up and lifted Lundqvist's mask and shield, exposing Lundqvist's neck at the moment the high shot needed to be saved. The play can be seen below:

Lundqvist squirmed on the ice in obvious pain after taking the puck directly to his unprotected neck. Rangers trainer Jim Ramsay immediately started to pick up snow from the ice and apply to to Lundqvist's neck to relieve pain and swelling. After a few quick diagnostic tests (probably a concussion screen, Lundqvist shook off the pain and continued to play. Video of the whole incident can be seen below:
On January 31st in a game against the Carolina Hurricanes, Rangers defenseman Ryan McDonagh attempted to clear the crease. Doing so, McDonagh's stick inadvertently came up and lifted Lundqvist's mask and shield, exposing Lundqvist's neck at the moment the high shot needed to be saved. The play can be seen below:

Lundqvist squirmed on the ice in obvious pain after taking the puck directly to his unprotected neck. Rangers trainer Jim Ramsay immediately started to pick up snow from the ice and apply to to Lundqvist's neck to relieve pain and swelling. After a few quick diagnostic tests (probably a concussion screen, Lundqvist shook off the pain and continued to play. Video of the whole incident can be seen below:
The next day Lundqvist tweeted that he was fine and even joked a bit:
Lundqvist recovered and started the next game on February 2nd. Lundqvist hasn't played since and on February 6th the Rangers announced he had a vascular injury and would be out 4-6 weeks.
THE INJURY
On Wednesday, February 4th, Rangers coach Vigneault told the media Lundqvist was being evaluated by doctors. On Friday, the 6th, it was released that he would be sidelined for at least 4 weeks with a neck injury and speculation begun (was it a concussion? was it nerve damage? a blood clot?). Then it was revealed that Lundqvist had a vascular injury and the hockey world promptly started googling and freaking out. Artery injury?! Risk of stroke! Woah! The NHL has certainly had its fair share of serious and bizarre injuries over the past year, and even experienced stroke with star defenseman Kris Letang (which I wrote about here).
On February 8th, Lundqvist spoke to the media and said he "sprained a blood vessel" (not a real medical term) and that he was risking a stroke had he continued to play, admitting it wasn't a good decision to play on the 2nd, the game following his injury. Lundqvist also said that he felt lightheaded, dizzy, and experienced headaches after taking the shot to the neck.
So what is a vascular injury? Essentially, it's an injury to the blood vessels/arteries. Lundqvist took a shot to the neck, a vulnerable area because it's where the blood vessels which provide [oxygenated] blood to the brain are located. In Lundqvist's case, his vascular injury wasn't very traumatic - meaning his vessels weren't torn or cut (Clint Malarchuk anyone?). However, the direct impact did cause blunt trauma to his neck's blood vessels resulting in damage manifesting in some of the symptoms that he reported.
Given the placement of where the puck hit (front/anterior of neck), it's most definitely an injury to the carotid artery. The carotid artery, known as the common carotid artery, is a paired structure meaning that there are two, one on each side of the body/neck. The left carotid artery originates from the aortic arch while the right originates in the neck from the brachiocephalic trunk. These arteries supply the head and neck with oxygenated blood, dividing in the neck to form the external and internal carotid arteries. The internal carotid artery directly supplies the brain, while the external carotid brings blood to other portions of the head such as the face, scalp and skull.

In the time following his injury, Lundqvist revealed that his neck was stiff, he had continued headaches, and felt light-headed. The stiff neck is a consequence of trauma to the neck muscles, and should resolve with a common regimen of ice & rest. The light-headedness, dizziness & headaches is what's concerning & is a direct result of his vascular injury.
Lundqvist suffered a vascular injury, meaning the trauma caused the structural integrity of the arterial wall to be compromised. In medicine, this is commonly known as an arterial dissection (Liebeskind & Saver). A dissection occurs with separation of the arterial wall layers, allowing blood to collect between layers (known as an intramural hematoma). When the interior arterial wall separates, it causes a false lumen to arise in the space where blood can seep into the vessel wall as seen below:
When a dissection occurs, the arterial wall is thinner, and susceptible to causing the blood vessel to enlarge and/or form a clot. Blood can still flow through the vessel to provide oxygen to the brain, but the structure is weakened.
The frightening [small, but definite] risk with a carotid dissection, as Lundqvist mentioned, is a stroke. A clot can form over the vessel wall where it is separated and naturally healing. Said clot could break and dislodge, forming an emboli, which could travel to the brain and disturb the flow of blood supply, resulting in an ischaemic stroke. Dissection is a common cause of stroke in young adults, accounting for up to 25% of all stroke cases.
DIAGNOSING THE INJURY
While clinical features (such as headache, dizziness, even tinnitus) may raise a physician's suspicion for dissection, the actual diagnosis can only be made and confirmed with neuroimaging. Imaging must demonstrate one of a couple features to make a diagnosis; a long tapered arterial stenosis, a tapered occlusion, a dissecting aneurysm (pseudoaneurysm), an intimal flap, a double lumen, or an intramural hematoma (Liebeskind & Saver).
After reporting his symptoms, Lundqvist presumably had a physical examination paired with an MRI/CT of the head and neck. While those two aren't used to diagnose a dissection itself, they aid in ruling out other possible injuries and point to the need to get more imaging, specifically those which provide images of the blood vessels.
Noninvasive imaging approaches such as Magnetic Resonance Angiography (MRA) and Computed Tomography Angiography (CTA) are the industry standard for diagnosing dissections and guiding treatment decisions. In fact, a 2009 study showed that both MRAs and CTAs diagnosis arterial dissections with relative similarity (http://www.ncbi.nlm.nih.gov/pubmed?term=19770343). Sometimes, a team of physicians will perform an MRA first, and then a follow-up CTA to confirm diagnosis.
In his case, Lundqvist's imaging most likely showed an abrupt narrowing of the [right] internal carotid artery, warranting an MRA/CTA. Lundqvist's MRA would then demonstrate a segment of dissection, most likely observed due to an intimal flap. When the internal lining of an artery tears, the blood (flowing at a high pressure) travels through the media as described above; this creates a false lumen (a newly created passageway). The false lumen is separated from the "true lumen" by a layer of tissue, which is known as the intimal flap.
TREATMENT & PROGNOSIS
Lundqvist must rest and avoid any straining or twisting of the neck. He probably resumed light cardio exercise already, but must limit his neck motion and any possible contact to the neck.
The good news is that dissections heal on their own. In most cases, arteries with luminal irregularities caused by spontaneous dissection undergo recanalization (restoring normal flow) and healing in the first few months after the event (Liebeskind & Saver). Lundqvist will be re-evaluated and have follow-up imaging to determine the progress of his healing somewhere around the 4-week mark after the injury.
Most patients with a carotid dissection are placed on an anticoagulant (blood thinner), which I've discussed at length in my pieces on Rinne, Letang, and Vokoun. Patients will be placed on a 4-6 week regimen of the blood thinner, and due to an increased risk of bleeding (especially in a sport like hockey), athletes on anticoagulants aren't allowed to play. However, Lundqvist noted that he wasn't taking an anticoagulant but rather [daily] full-dose Aspirin, which does have [less-potent] anticoagulant properties and is relatively safe.
The main factor in Lundqvist's recovery is how fast his blood vessel can heal, and if he sticks to a strict regimen of rest to avoid potentially re-injuring himself. Yes, there is a small but definite risk of stroke, but in Lundqvist's case, it's great they caught the injury fairly early and he seems to be aware of the risk.
SOURCE:
At least I saved it 👍 I'll prob stick to soup today, feel pretty good though. Thanks for all the well wishes! pic.twitter.com/2xTTHVkTUA
— Henrik Lundqvist (@HLundqvist30) February 1, 2015
Lundqvist recovered and started the next game on February 2nd. Lundqvist hasn't played since and on February 6th the Rangers announced he had a vascular injury and would be out 4-6 weeks.
THE INJURY
On Wednesday, February 4th, Rangers coach Vigneault told the media Lundqvist was being evaluated by doctors. On Friday, the 6th, it was released that he would be sidelined for at least 4 weeks with a neck injury and speculation begun (was it a concussion? was it nerve damage? a blood clot?). Then it was revealed that Lundqvist had a vascular injury and the hockey world promptly started googling and freaking out. Artery injury?! Risk of stroke! Woah! The NHL has certainly had its fair share of serious and bizarre injuries over the past year, and even experienced stroke with star defenseman Kris Letang (which I wrote about here).
On February 8th, Lundqvist spoke to the media and said he "sprained a blood vessel" (not a real medical term) and that he was risking a stroke had he continued to play, admitting it wasn't a good decision to play on the 2nd, the game following his injury. Lundqvist also said that he felt lightheaded, dizzy, and experienced headaches after taking the shot to the neck.
So what is a vascular injury? Essentially, it's an injury to the blood vessels/arteries. Lundqvist took a shot to the neck, a vulnerable area because it's where the blood vessels which provide [oxygenated] blood to the brain are located. In Lundqvist's case, his vascular injury wasn't very traumatic - meaning his vessels weren't torn or cut (Clint Malarchuk anyone?). However, the direct impact did cause blunt trauma to his neck's blood vessels resulting in damage manifesting in some of the symptoms that he reported.
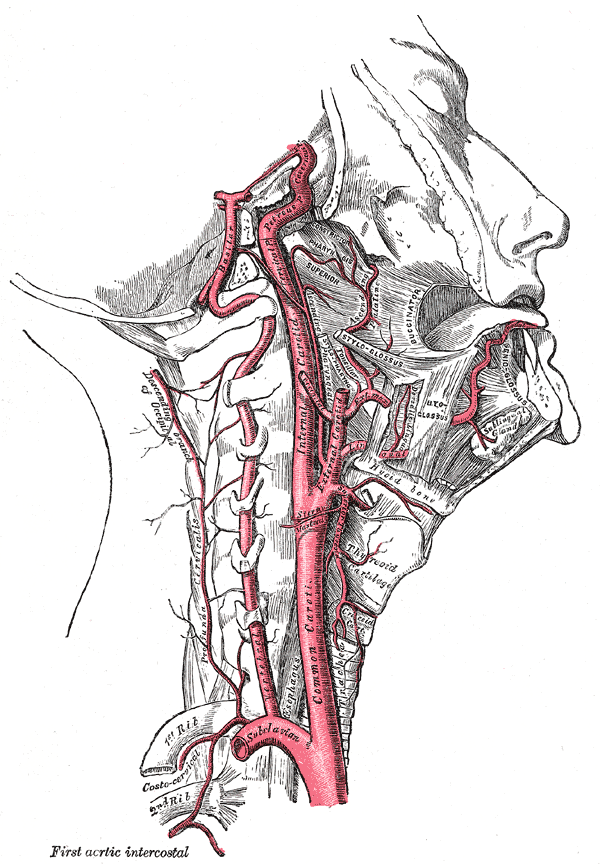 |
| The arteries of the neck [Wikipedia] |
Given the placement of where the puck hit (front/anterior of neck), it's most definitely an injury to the carotid artery. The carotid artery, known as the common carotid artery, is a paired structure meaning that there are two, one on each side of the body/neck. The left carotid artery originates from the aortic arch while the right originates in the neck from the brachiocephalic trunk. These arteries supply the head and neck with oxygenated blood, dividing in the neck to form the external and internal carotid arteries. The internal carotid artery directly supplies the brain, while the external carotid brings blood to other portions of the head such as the face, scalp and skull.

In the time following his injury, Lundqvist revealed that his neck was stiff, he had continued headaches, and felt light-headed. The stiff neck is a consequence of trauma to the neck muscles, and should resolve with a common regimen of ice & rest. The light-headedness, dizziness & headaches is what's concerning & is a direct result of his vascular injury.
Lundqvist suffered a vascular injury, meaning the trauma caused the structural integrity of the arterial wall to be compromised. In medicine, this is commonly known as an arterial dissection (Liebeskind & Saver). A dissection occurs with separation of the arterial wall layers, allowing blood to collect between layers (known as an intramural hematoma). When the interior arterial wall separates, it causes a false lumen to arise in the space where blood can seep into the vessel wall as seen below:
 |
| The progression of a dissection, thrombus development, and total vessel occlusion. Courtesy of Dr. Mounzer Kassab, Up To Date. |
The frightening [small, but definite] risk with a carotid dissection, as Lundqvist mentioned, is a stroke. A clot can form over the vessel wall where it is separated and naturally healing. Said clot could break and dislodge, forming an emboli, which could travel to the brain and disturb the flow of blood supply, resulting in an ischaemic stroke. Dissection is a common cause of stroke in young adults, accounting for up to 25% of all stroke cases.
DIAGNOSING THE INJURY
While clinical features (such as headache, dizziness, even tinnitus) may raise a physician's suspicion for dissection, the actual diagnosis can only be made and confirmed with neuroimaging. Imaging must demonstrate one of a couple features to make a diagnosis; a long tapered arterial stenosis, a tapered occlusion, a dissecting aneurysm (pseudoaneurysm), an intimal flap, a double lumen, or an intramural hematoma (Liebeskind & Saver).
After reporting his symptoms, Lundqvist presumably had a physical examination paired with an MRI/CT of the head and neck. While those two aren't used to diagnose a dissection itself, they aid in ruling out other possible injuries and point to the need to get more imaging, specifically those which provide images of the blood vessels.
Noninvasive imaging approaches such as Magnetic Resonance Angiography (MRA) and Computed Tomography Angiography (CTA) are the industry standard for diagnosing dissections and guiding treatment decisions. In fact, a 2009 study showed that both MRAs and CTAs diagnosis arterial dissections with relative similarity (http://www.ncbi.nlm.nih.gov/pubmed?term=19770343). Sometimes, a team of physicians will perform an MRA first, and then a follow-up CTA to confirm diagnosis.
 |
| Using imaging together - On the left is an MRI of the brain, showing a hemorrhagic crescent. On the right is a neck MRA, showing "string sign" consistent with dissection. (Source: Pary LF, Rodnitzky RL. Traumatic internal carotid artery dissection associated with taekwondo. Neurology 2003; 60:1392) |
 |
| A basic MRA image of the carotid arteries. |
In his case, Lundqvist's imaging most likely showed an abrupt narrowing of the [right] internal carotid artery, warranting an MRA/CTA. Lundqvist's MRA would then demonstrate a segment of dissection, most likely observed due to an intimal flap. When the internal lining of an artery tears, the blood (flowing at a high pressure) travels through the media as described above; this creates a false lumen (a newly created passageway). The false lumen is separated from the "true lumen" by a layer of tissue, which is known as the intimal flap.
 |
| A catheter angiogram showing an intimal flap (arrow) indicating dissection in an internal carotid artery. (Source: Suter B, El-Hakam LM. Child neurology: stroke due to nontraumatic intracranial dissection in a child. Neurology 2009; 72:e100.) |
Lundqvist must rest and avoid any straining or twisting of the neck. He probably resumed light cardio exercise already, but must limit his neck motion and any possible contact to the neck.
The good news is that dissections heal on their own. In most cases, arteries with luminal irregularities caused by spontaneous dissection undergo recanalization (restoring normal flow) and healing in the first few months after the event (Liebeskind & Saver). Lundqvist will be re-evaluated and have follow-up imaging to determine the progress of his healing somewhere around the 4-week mark after the injury.
Most patients with a carotid dissection are placed on an anticoagulant (blood thinner), which I've discussed at length in my pieces on Rinne, Letang, and Vokoun. Patients will be placed on a 4-6 week regimen of the blood thinner, and due to an increased risk of bleeding (especially in a sport like hockey), athletes on anticoagulants aren't allowed to play. However, Lundqvist noted that he wasn't taking an anticoagulant but rather [daily] full-dose Aspirin, which does have [less-potent] anticoagulant properties and is relatively safe.
The main factor in Lundqvist's recovery is how fast his blood vessel can heal, and if he sticks to a strict regimen of rest to avoid potentially re-injuring himself. Yes, there is a small but definite risk of stroke, but in Lundqvist's case, it's great they caught the injury fairly early and he seems to be aware of the risk.
SOURCE:
Liebeskind, D & Saver, J. Spontaneous cerebral and cervical artery dissection. In: UpToDate. Topic 14082 Version 16.0. Last Updated Feb. 10, 2015. UpToDate, Waltham, MA.
http://www.uptodate.com/contents/spontaneous-cerebral-and-cervical-artery-dissection-clinical-features-and-diagnosis
http://www.uptodate.com/contents/spontaneous-cerebral-and-cervical-artery-dissection-clinical-features-and-diagnosis
No comments:
Post a Comment