WHAT IS A CONCUSSION
Mild traumatic brain injury (mTBI), or concussion, is the most common type of traumatic brain injury/ While typically not too serious in most cases, concussion has a serious risk of short and long-term sequelae. At the 4th International Conference on Concussion in Sport (Zurich, November 2012), a panel discussion took place to obtain a consensus-based definition of a concussion. The Concussion in Sport Group (CISG) defined a concussion as follows:
Concussion is a brain injury and is defined as a complex pathophysiological process affecting the brain, induced by biomechanical forces. Several common features that incorporate clinical, pathologic and biomechanical injury constructs that may be utilised in defining the nature of a concussive head injury include:In essence, a concussion is a head injury with a temporary loss of brain function that may result in a variety of physical, cognitive, and emotional symptoms. Presently, concussion is a clinical diagnosis based largely on the observed injury mechanism (point of contact, force on head area, etc.), signs, and symptoms. The first step towards a diagnosis of a concussion is actual recognition of the injury.
The hallmark signs and symptoms of acute sports concussion include (but are not limited to):
- Loss of consciousness (LOC)
- However, the majority of concussions in sports occur without a LOC
- Problems with attentional mechanisms
- Manifested as (but not limited to): slowness to answer questions and follow directions, easily distracted, poor concentration, vacant stare/glassy eyed.
- Memory disturbance
- Balance disturbance
These symptoms may be apparent immediately after the head injury or other signs and symptoms of a concussion may evolve and appear gradually over several minutes. Additionally, over the course of the first 24 hours following a concussion injury, other signs and symptoms may manifest. However, it's important to note that there is a large range of these symptoms and they often vary, not all of these symptoms are seen in every case of sports concussion. The most common symptoms reported in concussion literature include:
- Somatic symptoms such as headache
- Cognitive symptoms such as feeling like in a fog
- Emotional symptoms such as lability
- Physical symptoms such as LOC and amnesia
- Behavior changes such as irritability
- Cognitive impairment
- Sleep disturbance (insomnia)
- Dizziness and balance problems
- Blurred vision
- Fatigue
I'd like to focus on amnesia because it will come into play later. Amnesia is a common physical symptom associated with mTBI. Amnesia almost always involves loss of memory for the traumatic event but frequently includes loss of recall for events immediately before (retrograde amnesia) and after (anterograde amnesia) the traumatic event.
Since concussions are often hard to recognize and to diagnose, the Zurich Consensus on Concussion in Sport proposed diagnostic criteria for sideline evaluation. An athlete shows any of the following, they need to be removed from play and assessed.
- Initial obvious physical signs consistent with concussion (LOC, balance problems)
- Teammates, trainers, coaches observe cognitive or behavior changes in functioning consistent with concussion symptoms reported
- Any concussion symptoms reported by the athlete injured
- Abnormal neurocognitive or balance examination
Following a removal from play:
- Physician evaluated the player using standard emergency management principles, most notably to exclude severe head trauma or cervical spine injury
- Once first aid issues are addressed, assessment of the concussive injury should be made using the SCAT3 or other sideline assessment tools (NHL uses ImPACT concussion testing, read here: http://www.impacttest.com/about/)
- The player should not be left alone following the injury and serial monitoring for deterioration is essential over the initial few hours following injury
- A player with diagnosed concussion should not be allowed to return to play on the same day.
- It has been unanimously agreed that an athlete should not return to play on the same day of the injury. Studies have shown that athletes allowed back into play following a concussion may demonstrate neuropsychological deficits post injury.
CONCUSSION MANAGEMENT AND RECOVERY
The graduated return to play protocol following a concussion is a stepwise process and is outline below:

CONCUSSIONS IN THE SPORT OF SOCCER
Most people associate concussions with violent/physical sports, specifically American football, hockey and boxing. Of all sports played in the United States, football is the sport associated with the greatest number of traumatic brain injuries, but it also has the largest number of participants.
In the US, soccer is a sport growing in popularity. Between 1982 ad 2008, approximately 7.2 million men and 5.2 million women played soccer at the high school level and an additional 430,000 men and 322,000 women at the college level (Cantu and Mueller).
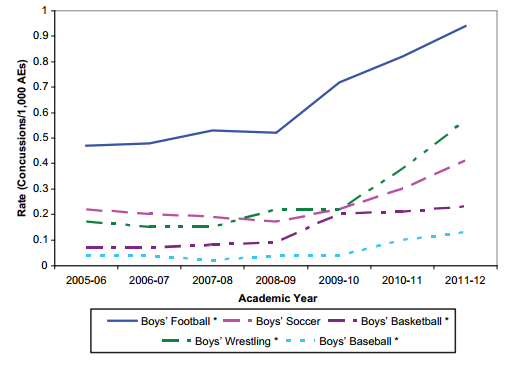
Recently, a study (Rosenthal et al) was published which analyzed data from High School Reporting Information Online (HS RIO), a national high school sports injury surveillance system. In this system, high schools across the nation with at least 1 certified athletic trainer were invited to participate. The trainers would log into the system and report injuries and athlete-exposures (AE) which was defined as 1 athlete participating in 1 competition or practice. The study used a sample of 100 schools for participation in the concussion rate study and focused on 9 sports: baseball, boys and girls basketball, football, boys and girls soccer, wrestling, softball and girls volleyball. These sports were chosen because data was available from 2005-2006 through 2011-2012.
The study reported the following rates:

"The HS RIO data showed a significant increase in overall concussion rate in the 7-year period of the study. The rates significantly increased in 5 of the 9 sports studied and showed increasing trends in the others. As can be seen from our results, the majority of the rate increase for all sports was observed after the 2008-2009 academic year."The graphs from the study shown below show total concussion rates for girls and boys sports from 2005-2006 through 2001-2012:

As you can see, the rate of concussions has increased in both boys and girls soccer. However, girls sustain a higher rate of concussions.
Another study (Gessel et al) also used the HSRIO data to survey the injury and drive targeted injury-prevention projects. The researchers determined that the risk factors for concussion in soccer differed significantly by sex. Concussions in soccer players most frequently occur as a result of head to head collisions in the act of heading the ball; 40.5% of the time in males and 36.7% in females. Girls soccer players sustain a greater proportion of concussions related to contact to the ground (22% compared to 6%) and contact with the ball (18.3% compared to 8.2%). Another risk factor for concussions in soccer is playing the position of keeper, with 21.7% of injuries to goalkeepers being concussions, compared with 11.1% of injuries to other positions.

Up to 50% of players admit to bending the truth about their symptoms to get back into action more quickly. It's imperative to teach them that a brain injury is not like any others, it could be irreversible. You can cause serious damage by not being honest about your symptoms and condition and by returning to play with a brain injury.
ALVARO PEREIRA - URUGUAY
During the group stage match between Uruguay and England, midfielder Alvaro Pereira took an inadvertent knee to the head from English winger Raheem Sterling. Pereira was attended to by medical staff who found him flat on his back and unresponsive.
 |
| Kirsty Wigglesworth/Associated Press |
After being attended to by the head physician and sideline medical team, Pereira regained consciousness and was helped to the sideline. The team doctor stepped away to signal to the manager that the stumbling Pereira should be substituted out. Pereira adamantly protested and made his way back onto the pitch just two minutes later.
At the very least, Pereira's condition merited a full evaluation by the team physician which can take at minimum seven minutes. In sports such as hockey and football, where concussion protocol is taken extremely seriously, the player would have had to exit the field/ice for a full evaluation and cleared, if not substituted for the rest of the game. Pereira's demand to play on should not overrule advice from the team physician for him to be substituted. Should the referee have intervened and not allowed him back on the pitch? In returning, Pereira put himself at risk for worse and possibly irrecoverable injury.
Pereira admitted his mistake after the match, apologizing to the doctor and stating that he "was dizzy," a sign of being concussed. Pereira said "the lights went out" after being hit in the head but wanted to play on to help the team. In the picture below, you can see that Pereira clearly looks groggy after regaining consciousness. All of these are telltale signs of a concussion.
 |
| Matthias Hangst/Getty Images |
JAVIER MASCHERANO - ARGENTINA
In the semi-final of Argentina v. Netherlands, another seemingly concussed player was allowed to return to the pitch and continue playing. While going for a header, Mascherano bumped heads with a Netherlands player, falling to the pitch and looking close to losing consciousness. After getting up, Mascherano couldn't walk straight, staggering around the pitch with a blank stare before trying to grab onto a Dutch player, missing, and falling to the ground.
Mascherano eventually walked off the pitch but only spent about two minutes on the sideline before returning for the rest of the match. While Mascherano was lauded for his performance the rest of the match, it's pretty clear he was at great risk of further injury and probably shouldn't have returned. As was the case with Pereira's injury, Mascherano returned to the pitch way too soon. A full neurological evaluation and concussion battery test takes at least six to seven minutes.
CHRISTOPH KRAMER - GERMANY
It was a dream start for 23-year-old German midfielder Christoph Kramer on Sunday. Despite playing in just 12 minutes in Brazil prior to the final, Joachim Löw elected to start Kramer after veteran Sami Khedira sustained a calf injury during warm-ups. Kramer's dream, however, was cut short after being struck in the head by Argentine defender Ezequiel Garay. Kramer laid on the pitch and was briefly evaluated by the German national team's physios. After a few minutes, Kramer returned to play but was eventually substituted in the 31st minute.
On the world's biggest stage, the FIFA concussion protocol was once again exploited and criticized around the world. Instead of Gotze's game winning goal being the most impactful image from the final, Kramer's dazed look will stick in the memory of fans around the world:
 |
| Thousand yard stare |
WHAT CAN BE DONE?
The negligence shown by FIFA and team physicians towards head injuries during the World Cup has caused a lot of debate. Every news and media source and online forums are talking about what can be done and which rule changes FIFA should implement to combat the problem.
What is clear though is that coaches are hesitant to substitute a player with a possible head injury due to the limited amount of substitutes available. Coaches and physio staff also allow players to return to the pitch too quickly because of the disadvantage of being down a man during the time which it takes to get a proper examination.
The most common suggestion is the addition of a fourth substitute, specifically in the case of a possible concussion. However, even if implemented perfectly by FIFA, the rule could be easily exploited by players faking a concussion in order to get an extra sub late in a match (players are already infamous for faking injuries to gain an advantage).
Another suggestion that absolutely should be implemented is the addition of an independent physician in international matches. A player would be less likely to fake an injury to an independent doctor rather than a team doctor. An independent physician would also be less biased and would want to fully evaluate the player before allowing him back on the pitch.
There isn't a perfect solution. However, FIFA's extremely poor concussion protocol was exploited on the biggest stage this past world cup and something needs to be changed. Physicians should know that if a player has suffered a concussion he should NEVER return to play. Players should be educated on the risks of head injuries along with coaches and staff. Substitutions should not be treated like gold, but rather the player's lives should be after they appear to suffer a head injury.
SOURCES:
Cantu RC, Mueller FO. The prevention of catastrophic head and spine injuries in high school and college sports. Br J Sports Med Dec;2009 43(13):981-986.
Gessel LM, Fields Sarah K, Collins CL, Dick RW, Comstock RD. Concussions Among United States High School and Collegiate Athletes. Journal of Athletic Training 2007;42(4):495-503.
Rosenthal JA, Foraker RE, Collins CL, and Comstock RD. National High School Athlete Concussion Rates from 2005-2006 to 20112012. Am J Sports Med 2014 Apr 16;42(7):1710-1715.
"Substitutions should not be treated like gold, but rather the player's lives should be after they appear to suffer a head injury."
ReplyDeleteYeah. We're surrounded by footballers that are disabled because their frequent concussions. Can't believe no one's cared until now. Oh wait, that's not true at all. I'm sick of this overstating what is in the grand scheme of things a minor risk. Educate the players and staff, absolutely. Managers are going to sub a player if they see he's a detriment on the pitch. But I guarantee most every player is going to choose to play if allowed even knowing the minor risks.
The point is prevention from a player one day dying due to an mTBI. The risks also are not minor but can cause long-term damage if not treated correctly.
DeleteFormer athletes around the world ARE affected by a history of concussions. This isn't a minor risk.
Also you're completely wrong about players lives not being affected by this. Alecko Eskandarian had his career cut short by concussions: http://www.nytimes.com/2014/07/16/sports/soccer/world-cup-2014-christoph-kramers-head-injury-brings-fifas-problem-to-the-forefront.html
DeleteAs did Taylor Twellman. There’s a story about how, for his final game, he took a laundry list of painkillers and shotgunned a beer before taking the field.
Individual scare stories don't move me OK, there's two people. And there are probably hundreds more. Out tens of thousands that have played football. And I'm sure that someday someone will die of a mTBI on the pitch someday. I'm not sure the exact delineation between mild or not, but there are around 10 documented deaths due to on the pitch head injuries. A few more than from lightning strikes. It just doesn't ring as such a massive risk that demands this kind of outrage and changes to how the game has been played for decades.
ReplyDelete